There’s mixed opinions regarding artificial sweeteners in the ketogenic world, with some cautioning against their use. One common concern is that they can cause a rise in blood insulin levels, which is something we are specifically trying to avoid by restricting carbohydrates.
I’ve been eating low carb / keto for about 19 years now, and lost, and kept off, 90 pounds. My wife has been even more successful over a shorter time period, losing 175 pounds. Both of us use artificial sweeteners, either in the form of diet soda or adding it to foods we make (and in her case keto friendly things she bakes).
Were we just lucky? I wanted to see whether there was any scientific evidence supporting the view that they raise insulin levels. A Google search turned up numerous pages advising against using artificial sweeteners. Most were unsourced, but quite a few did reference another website or a book, for example Dr. Jason Fung’s The Obesity Code, so I decided to start there. From chapter 15:
The important question is this: Do artificial sweeteners increase insulin levels? Sucralose(13) raises insulin by 20 percent, despite the fact that it contains to calories and no sugar. This insulin-raising effect has also been shown for other artificial sweeteners, including the “natural” sweetener stevia. Despite having a minimum effect on blood sugars, both aspartame and stevia raised insulin levels higher even than table sugar.(14) Artificial sweeteners that raise insulin should be expected to be harmful, not beneficial. Artificial sweeteners may decrease calories and sugar, but not insulin. Yet it is insulin that drives weight gain and diabetes.
Jason Fung, The Obesity Code, Chapter 15, page 172
Next, I read these two studies myself, to see if they really justified the concerns over use of these sweeteners, specifically do they cause a rise in blood insulin levels for people eating a low carb / ketogenic diet. Here are the papers in question, along with links to the papers themselves. I’d suggest reading them before moving on to my interpretation of the studies:
13: Pepino et al: Sucralose Affects Glycemic and Hormonal Responses to an Oral Glucose Load. Diabetes Care 2013 Sep; 36(9): 2530–2535. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3747933/
14: Anton et al: Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetite. 2010 Aug; 55(1): 37–43.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2900484/
In the first study, Sucralose Affects Glycemic and Hormonal Responses to an Oral Glucose Load, seventeen obese test subjects drank either sucralose or regular water, and then underwent a standard five hour oral glucose tolerance test. This test measures the subject’s glucose level after fasting (as a baseline) and then after drinking a glucose solution (essentially sugar water), and was historically the standard test for diagnosing diabetes. Their blood glucose level is measured over five hours. In subjects without diabetes, their blood glucose level rises and falls quickly, in those with diabetes or an impaired glucose tolerance the blood glucose levels rise higher, and remain elevated for a longer time period. In this study, the subject’s blood insulin level was also measured, in addition to blood glucose.
The first graph, below, shows the blood glucose level of the subjects during the experiment as two lines, one for those who first drank water, as well as for those who first drank sucralose.
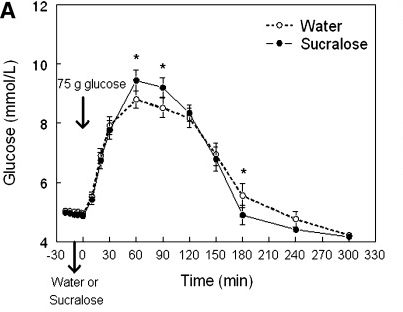
Up until time 0, when the oral glucose was administered, the blood glucose level was the same for both sets of test subjects. After administering the oral dose, the blood glucose levels went up as you would expect, although the peak value was higher for those who had sucralose first (more about this later!)
Next we have a graph of their blood insulin levels:
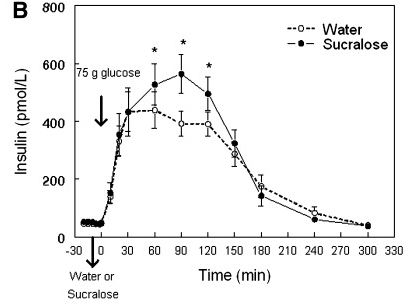
Again both graphs overlap before administering the glucose, implying that the sucralose did not cause a spike in blood insulin levels. As with the peak blood glucose level, the peak insulin level was higher for those who had sucralose prior to glucose. In both cases, think of the sucralose as having a multiplier effect on the later dose of glucose. What is going on here?
My suspicion is that the sweet taste of sucralose is priming the body to get ready digest food. Think back to Pavlov’s famous experiment with dogs, where they started to salivate when the bell was rung, the saliva contains enzymes that help break down food. If there’s an larger supply of these enzymes and other compounds available, it could facilitate faster absorption of the glucose. And indeed there is a phenomena known as cephalic phase insulin response (CPIR) which could be at play here, which I will also address further down.
If you’re eating a ketogenic or low carb diet, this would not be an issue, since you’re not eating carbohydrates, not more than very small amounts anyway. Remember how I considered the sucralose as having a multiplier effect on the blood glucose and insulin response? If you’re not eating carbohydrates, you’re not going to have a response. And anything multiplied by zero is still zero. So this isn’t going to affect you.
But if you’re eating the SAD (Standard American Diet) full of sugars and other carbohydrates, it’s quite plausible that drinking a diet soda along with your giant fries and burger could spike your insulin levels higher than if you just drank a glass of water. Of course the burger and fries alone would do that, but the diet soda might make it even worse. You can also argue that drinking a sugar filled non-diet soda would be just as bad or likely even worse due to its high sugar content.
But the key takeaway point for us, again, is that on a keto diet, it’s a non issue, as we are not eating a sugar or starch filled meal along with our diet soda. For example, if you eat a few eggs and some cheese, let’s say with 5g of carbohydrates, then a 20% increase in insulin levels would make that meal equivalent to eating 6g of carbs instead. It’s certainly something to factor into your daily meal planning, but is it significant? Further down I discuss CPIR, including a study that suggests other tastes may also trigger an insulin response prior to eating any carbohydrates, even those not from sweeteners. You may get the increase in insulin levels from eating virtually anything.
The second study, Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels, is used to support the claim that aspartame and stevia raise insulin levels, and indeed raise them higher even than table sugar. Let’s take a look at the study.
In the study, 31 individuals, 12 of whom were obese, participated in an experiment to see if substituting low calorie sweeteners for sugar would help with weight management. Stevia and aspartame were the low calorie sweeteners used, in addition to sucrose (regular sugar). The purpose of the experiment was not to see if these sweeteners adversely affected blood insulin levels, although blood insulin levels measurements taken during the trials have been used to support that claim.
The subjects fasted for 12 hours, arrived at the test center, and were fed a 469 kcal breakfast of cereal, milk, toast with butter, and orange juice. Then they were fed a 400g “preload” of tea and crackers with cream cheese sweetened with either stevia, aspartame, or sucrose 20 minutes before their test lunch or dinner meals.
The lunch meal was sandwiches, potato chips, and cookies. The dinner meal was a “self-selected buffet-type meal” (the details are in the paper, it too was just as high carb as lunch). So both meals were SAD (Standard American Diet), not keto. The subjects were allowed to eat as little or much of each meal as they liked, and reported their hunger and satiety levels. Again, recall the purpose of this experiment was not to see the effect of low calorie sweeteners on blood insulin levels, but whether or not they could be used in a diet to limit overall food/calorie consumption. I won’t dwell too much on the experiment results since they’re not relevant to the insulin effects other than to note that “Reported hunger and satiety levels did not differ by condition at any time point” even though they ate “significantly fewer kcal”.
The paper concludes “In conclusion, participants did not compensate by eating more at either their lunch or dinner meal and reported similar levels of satiety when they consumed lower calorie preloads containing stevia or aspartame than when they consumed higher calorie preloads containing sucrose.” Sounds to me like it was a success. Low calorie sweeteners can be helpful for people trying to diet and reduce weight. And these subjects were not even eating a low carb or keotgenic diet!
So back to the original ketogenic diet related claim, “Despite having a minimum effect on blood sugars, both aspartame and stevia raised insulin levels higher even than table sugar” and therefore should not be consumed on a low carb / keotgenic diet.
Blood insulin levels were measured before the “preload” meal, after it, as well as before and after the lunch meal. Figure 3 from the paper shows these blood insulin levels:
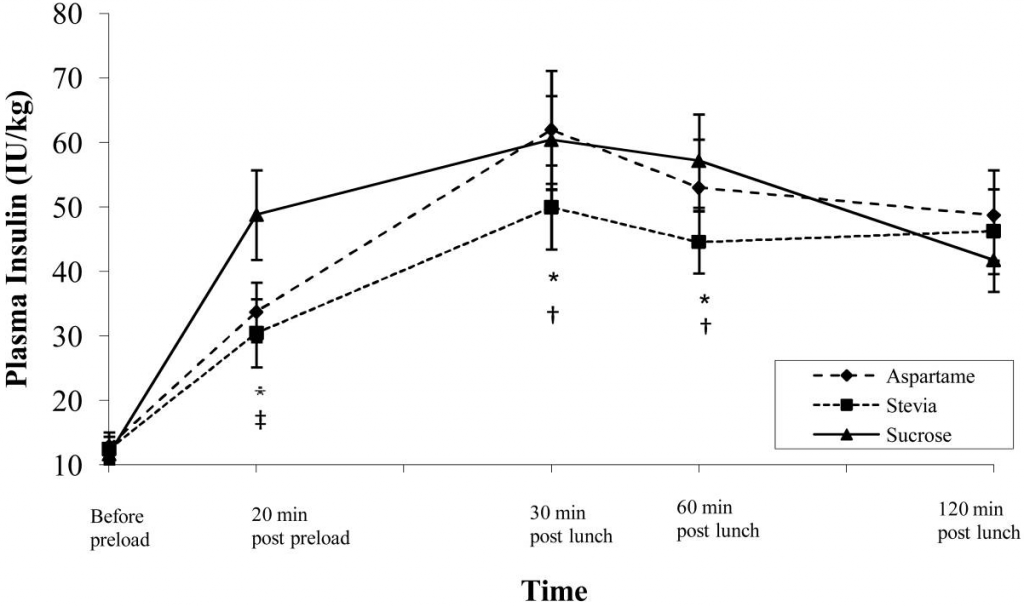
In all three cases (Stevia and aspartame, as well as regular sugar/sucrose) blood insulin levels went up after the preload. But wait, what was in this preload? Crackers with cream cheese! They did not consume just aspartame or stevia, they consumed it along with crackers.
The cracker and cream cheese meal with stevia and aspartame was reported as 290 kcal, unfortunately the paper does not specify the nutritional information for it, so we don’t know the sugar content. Crackers have a very high glycemic index, typically in the range of 67-81. Foods typically affect blood sugar levels by their glycemic index as a percentage relative to pure glucose – a large amount in this case.
Therefore, it’s not surprising the subjects had a blood insulin response. But don’t blame the aspartame or stevia for what the crackers did. At the end of the two hour measurement period, the insulin levels were approximately the same for all three cases, with the two low calorie sweeteners indeed slightly higher. But this was after eating a non keotgenic / high carb / SAD lunch. I find it difficult to believe this is relevant for someone eating keto.
As you can see in Figure 2 from the paper, aspartame and stevia did indeed have less of an effect on blood sugars than plain sugar/sucrose:
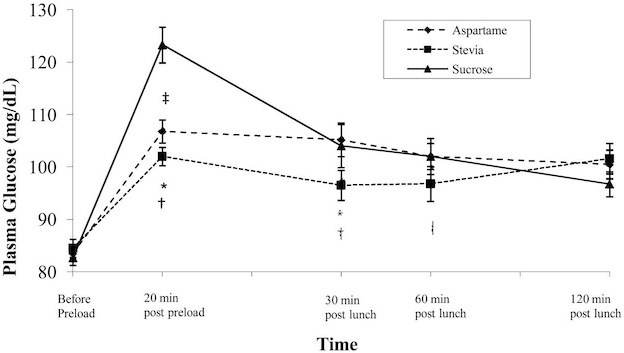
This is to be expected, since in those cases the subjects consumed less carbohydrate (they did not eat the sugar in addition to the crackers), and less insulin needed to be released by their body to deal with it.
It is worth repeating again, in this experiment the subjects did not consume just aspartame or stevia. They ate crackers and cream cheese, with either of those sweeteners or with regular sugar. That is why their insulin level went up. This study does not confirm that aspartame or stevia causes blood insulin levels to increase. It does however confirm that use of low calorie sweeteners does not cause an increase in calorie consumption, suggesting that they can be appropriate for a keto lifestyle.
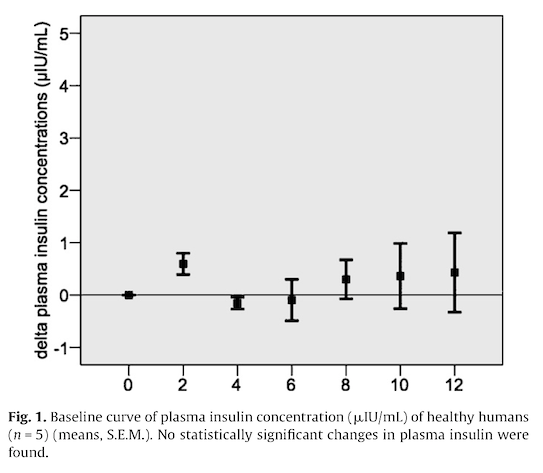
Earlier I mentioned cephalic phase insulin response (CPIR), which is the release of insulin prior to an increase in the blood sugar level. One paper which presents human experimental results is Just et al: Cephalic phase insulin release in healthy humans after taste stimulation? Appetite. 2008 Nov;51(3):622-7
https://pages.ucsd.edu/~mboyle/COGS163/pdf-files/Cephalic%20phase%20insulin%20release%20in%20healthy%20humans%20after%20taste%20stimulation-2008.pdf
Two studies were performed, a pilot with five subjects and a second with 20 subjects. In each study the subjects tasted (swished in their mouths but did not swallow) a specific taste while their blood glucose and insulin levels were measured: before the taste test and 3, 5, 7 and 10 minutes after.
In the pilot study, the subjects tasted starch, quinine (bitter taste), citric acid (sour), distilled water, MSG (umami) NaCl (table salt). The second study had two sweet tastes, sucrose (table sugar) as well as saccharine.
The glucose readings were relatively stable for all of the readings, while the insulin levels had more noticeable changes. (See Table 1 in the study) Insulin levels increased slightly for the sucrose and saccharine tests. But they also increased for quinine, starch, and even the plain distilled water (the latter two dismissed in the paper due to “outliers”). Curiously the insulin readings (both before and after tasting) for the salty taste were all significantly lower than for the other tastes, about 5.0 vs 8.5. Also the sour taste run had somewhat higher values, 11.0 vs 8.5. From the paper “The taste solutions were given in a randomized order, each solution was presented on a separate day.” This suggests to me that there could have been an offset error in the insulin readings for those two days. I’m not sure if it affects the validity of the results, but it is suspicious.
In addition, as an engineer with a background in process control, the insulin readings look extremely “noisy”to me. In addition to the large standard deviations in the values in Table 1, the baseline measurements where the fasting insulin level was measured every 2 minutes shows a continuously increasing variation in readings between subjects. Is this a measurement error, or because human insulin levels are continuously varying, perhaps to control blood glucose? How much of this noise is being added to any actual variations driven by the tastes?
While the paper focused on the effects of sucrose and saccharine, other tastes also produced an effect. Does the body only release a small amount of insulin when sweet is tasted, or does this occur for multiple tastes? All tastes? If so, it doesn’t matter what you eat, you will have a small increase in your blood insulin level, even if it’s not a sweetener. Regardless, the changes in insulin levels in all cases was small, in the case of saccharine around 11%. Remember from the earlier oral glucose experiment, the change was significantly larger, the 75g glucose load caused an approximately 1000% increase in insulin levels. This doesn’t proscribe the use of low calorie sweeteners by individuals on a ketogenic diet who are trying to control their blood insulin levels.
Control systems (sorry, I have my engineer hat on again) use a mix of feedback and feedforward for regulation. It’s probably not surprising that the body slightly increases insulin levels in anticipation of blood glucose levels possibly rising after eating, in addition to any releasing insulin when glucose levels do rise. In pre modern times, there were few if any sources of food that contained a large amount of sugar that would dramatically raise insulin levels, how often did our ancestors successfully raid a honeybee hive? The small bump in insulin would be sufficient for a few wild berries, root vegetables, etc. The insulin feedforward system may be coarse enough to respond to virtually any taste / food source, not just sweet.
My conclusion: The studies cited supporting the belief that artificial sweeteners significantly raise insulin levels on a keto diet don’t actually show that.









